No content results match your keyword.
Content
You have successfully logged out.
Not registered yet?
Vascular access
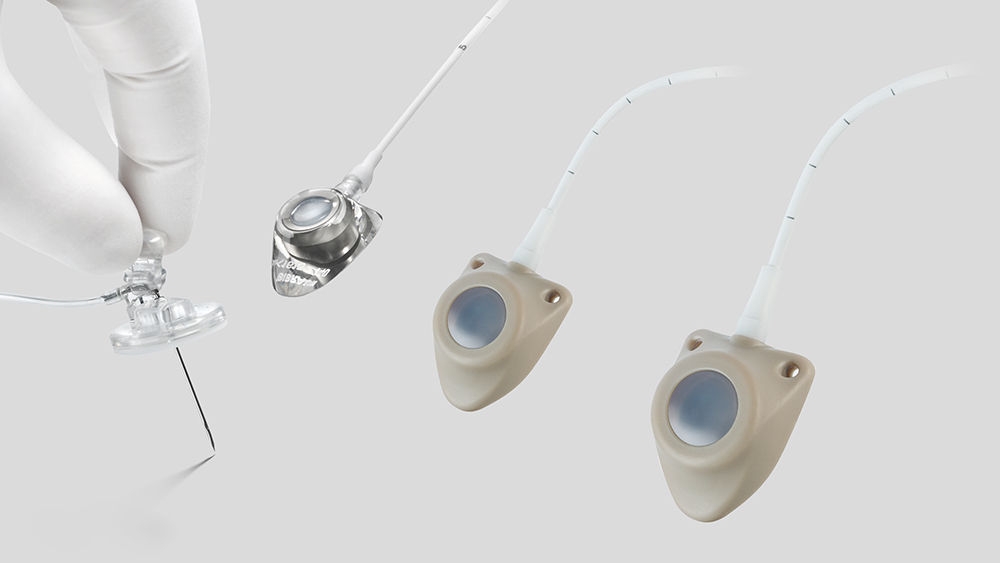
Access port catheters and port needles ensure easy vein access, reduce the risk of infections and improve patient comfort as well as quality of life. For long-term venous access without compromising safety.
A vascular access port device consists of a catheter connected to a reservoir. It is implanted subcutaneously and namely used to deliver drugs into the blood stream. Port access has become essential for venous, arterial, peritoneal, pleural, and spinal (epidural/intrathecal) access indications and is recommended for long-term therapies of more than 3 months. One of the main reasons for using a port access is to spare the patient repeated injections or infusions into one of the peripheral veins. The port implantation time depends upon the duration of the individual treatment.
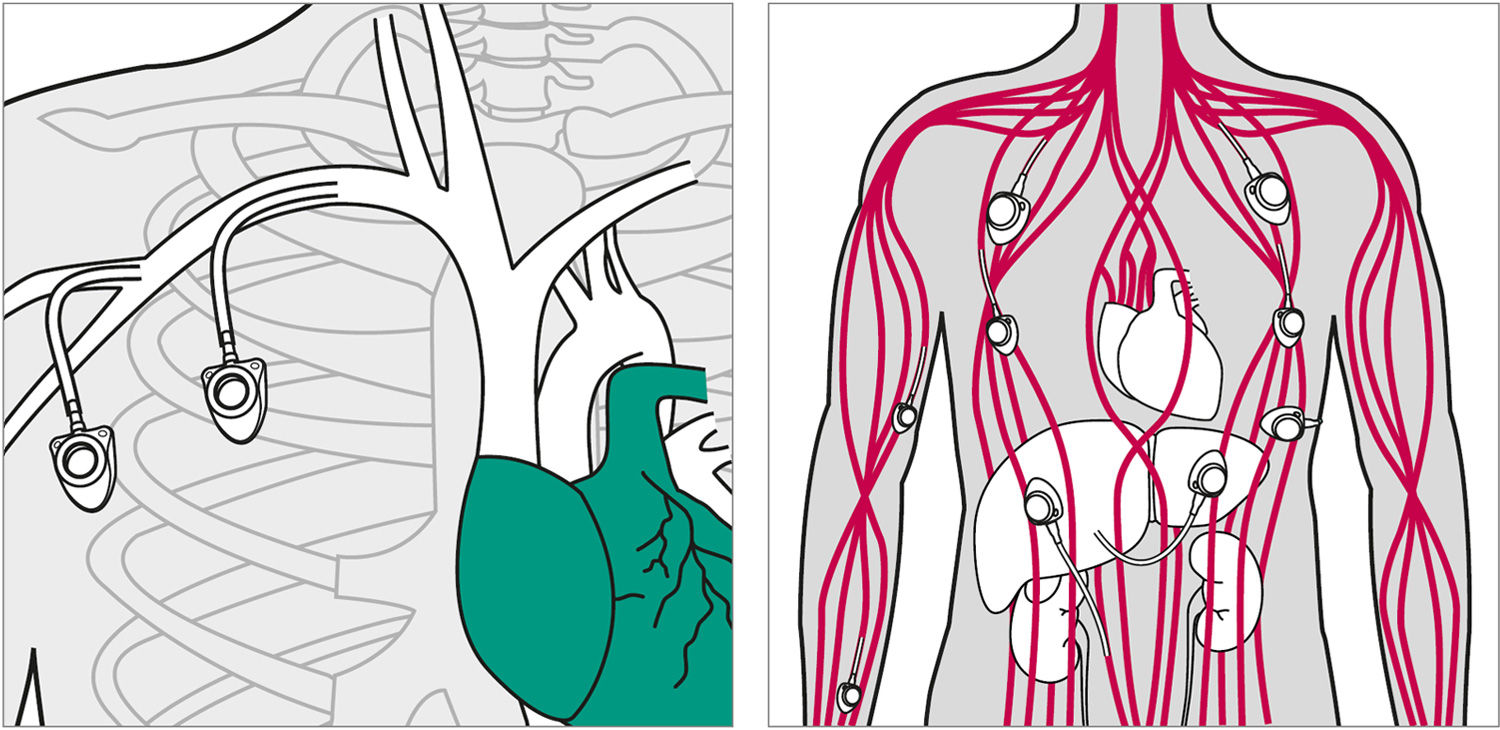
The implantation site is chosen according to the indication, clinical condition of the patient, the patient’s lifestyle and the treatment to be administered. The operation is simple and takes only around 30 minutes under local anesthesia (general anesthesia for children). The vascular access port may be placed in the upper or lower thoracic position or even in a brachial position with a dedicated brachial port.
The vein is punctured to introduce the catheter and the skin is incised to make a pocket to place the vascular access port under the skin. The port pocket is made as small as possible (about 2.5 cm). After implantation a dressing is placed to protect the incision. If treatment is required right after the port placement, it is possible for the physician to place immediately a needle into the port to administer the treatment.
If the treatment requires a few days infusion, a special needle will be put in place and covered with a sterile dressing. This needle does not need to be changed every day, but the maximum duration of needle placement should not exceed 7 days. When the patient is not receiving regular treatment through the access port, it is recommended to be flushed every 4 weeks. This is to make sure that the catheter and port are still functional. In most cases, there are no complications.
The insertion of the needle into the port is generally painless. However local anaesthetic cream can be applied over the injection site to numb the area. The access, use and maintenance of the vascular access port must be done according to strict aseptic rules and following approved local protocols.
There are many potential access routes for a central venous vascular access port catheter. The most used are the internal or external jugular veins, the subclavian vein, the cephalic vein and the axillary vein.

A vascular access port consists of an implantable catheter linked to a reservoir. The device is placed subcutaneously and can be used over a long time period for many types of infusions. Vascular access ports have considerably facilitated the development and security of general ambulatory treatment, especially in home care. They have also largely improved patient comfort.
It is of primary importance that the nursing staff takes care for hygiene precautions and follows the port usage process according to local protocols.
Rigorous aseptic rules must be followed, according to the given protocol of the hospital based on national and/or international guidelines to prevent infection of the access port. To avoid any contamination of the injection site, it is important to ensure that the patient’s head remains turned away from the site during the procedure and refection of the dressing.
Always verify that the access port and catheter are functional by aspirating blood into the syringe and injecting 10 mL (or 5 mL for children) of saline solution (NaCl) 0,9 % into the access port/catheter before starting the infusion.
As part of port maintenance, rinsing is required before starting a treatment, after each treatment, before changing the infusion solution and every four weeks when the system is not in use. This applies regardless of whether it is a venous catheter, an arterial catheter, an epidural/intrathecal catheter or a pleural catheter.
Flushing with heparinised saline solution (NaCI) 0.9 % can follow if required by local protocol. When heparinised saline solution (NaCI) 0.9 % is used, the system should be rinsed with 10 mL of saline solution (NaCI) 0.9 % alone before rinsing with heparinised saline (NaCl) 0.9 %. Some drugs react with heparin and may result in blockage of the access port/catheter due to formation of precipitates.
To avoid blood inside in the catheter, the port is flushed with normal saline solution (NaCI) 0.9 %. There is no specific recommendation regarding the removal technique of the needle.
The use of positive pressure or not, upon withdrawal of the needle, does not prevent blood diffusion into the lumen of the catheter over time. More important is to rinse the port and catheter as recommended in the Celsite® IFU’s, before, in between and after each infusion.
Brochure
Celsite®, Surecan®, Cytocan® – Access port systems, accessories and non-coring port needles
pdf, 6.0 MB
Nursing guidelines
Celsite® access ports – nursing guidelines for use and maintenance
pdf, 1.2 MB
Patient guide
Celsite® access port system
pdf, 729.9 KB
Celsite® Safety
Venous access port system
pdf, 803.0 KB