No content results match your keyword.
Content
You have successfully logged out.
Not registered yet?
No content results match your keyword.
Content
No product results match your keyword.
Products
Solutions beyond fusion
The Ennovate® Cervical system supports surgeons to achieve optimal surgical outcomes in the occipital, atlantoaxial, subaxial and upper thoracic region.
With our comprehensive spinal system we aim to offer the full range of possibilities – not only with additional navigation, but also for future-oriented technologies like the MIS approach. The system is structured into dedicated instrument modules, so you only open the instrument sets you truly need. Ennovate® Cervical combines next generation implants and instruments with lean process workflows to provide smart solutions for you.
Ennovate® Cervical MIS
Similar to minimally invasive stabilisation of the thoracolumbar spine, which has been proposed to reduce access-related morbidity such as muscular denervation, atrophy, length of hospital stay, blood loss and post-operative pain, [1-4] procedures for posterior cervical instrumentation represent the next logical step. Several pioneers already reported minimally invasive posterior procedures for stabilisation of the cervical spine. [5-9] The MIS module of the Ennovate® Cervical system offers dedicated navigation-ready instruments and implants allowing for a less invasive approach to the cervical spine with the goal to reduce access related morbidity such as post-operative pain.

Percutaneous cervical pedicle screw placement is challenging due to complex anatomy and requires navigation support. For this feasibility study in six cadavers, all subaxial cervical pedicles were fitted with screws using a standardised procedure. The results of the study indicate that percutaneously placed cervical pedicle screws can be inserted with a high grade of accuracy.
Read moreThis study reports on workflow and initial outcomes using a new exclusively minimally invasive surgery (MIS) approach for cervical pedicle screw (CPS) insertion. First clinical impressions of the market-ready Ennovate® Cervical system using iCT navigation are shared. The outcome of a series of ten patients is presented. It is discussed, that for selected cases, MIS approach for CPS placement appears feasible and safe.
Read moreAs in the thoracic and lumbar spine, MIS techniques of the cervical spine strive to achieve results comparable to those of conventional procedures in terms of “target surgery”, while at the same time offering the advantages of less traumatizing “access surgery”. However, unlike in the thoracic and lumbar spine, MIS techniques on the cervical spine are predominantly used dorsally.
Read moreThis retrospective case series included patients with cervical instabilities treated by minimally invasive percutaneous cervical an upper thoracic spine pedicle screws and rod insertion with Ennovate® Cervical. The results of this study indicate that minimally invasive percutaneous implantation of a pedicle screw-rod system is feasible.
Read more
“With Ennovate® Cervical I have the full range of possibilities for solving complex situations I face in the operating room – It is a truly future-oriented system taking advanced minimally invasive approaches into account.”
Ennovate® performance design
Do you know what happens to the screws post-operatively? Long-term stability is often taken for granted and rarely considered in detail, since it is a primary requirement and assumed that it is technically impossible to get more out of a screw. Because screws are just screws. Well, we do not see it that way! Our German engineers have designed a screw that sets new biomechanical benchmarks.

Optimised bone purchase for enhanced pull-out strength through a harmonised drill and screw design.
/
All standard screws are canulated, offering the possibility to work with K-wires.
/
All screws accept both ⌀3.5 mm an ⌀4.0 mm rods for improved intraoperative flexibility and less inventory.
/
Standard polyaxial screws offer 45° in all directions. Additionally, favored angle screws offer 55° in the cranial and caudal plane.
/
Specially designed tip for deeper insertion, less insertion force and reduced risk of slipping.
/
Ennovate® Cervical EnnoCore
The Ennovate® Cervical implants have a specifically designed screw core and thread shape, all aiming to increase the stability and pull-out strength of the implants. But that´s not all: The drills are harmonized to meet the screw contour and are therefore designed to support better bone compaction and anchorage.
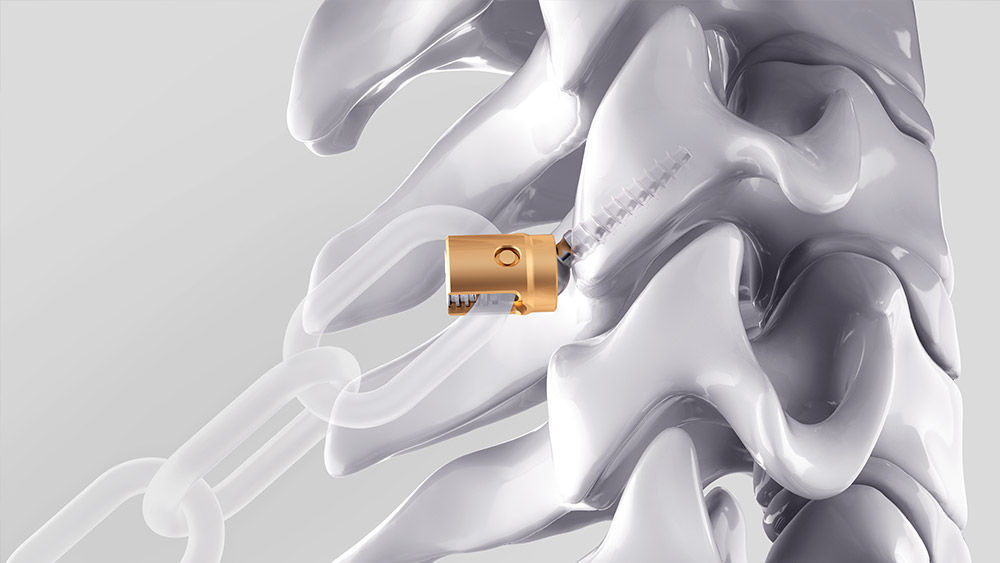
Ennovate® Cervical EnnoTip
The screw tip of the Ennovate® Cervical screw is specially designed to allow for a deeper initial insertion, thereby aiming to reduce the risk of slipping off the prepared bone. Furthermore, the thread starts directly at the screw tip, which is a design enabling a reduction of the required insertion pressure – critical in the highly mobile cervical spine.

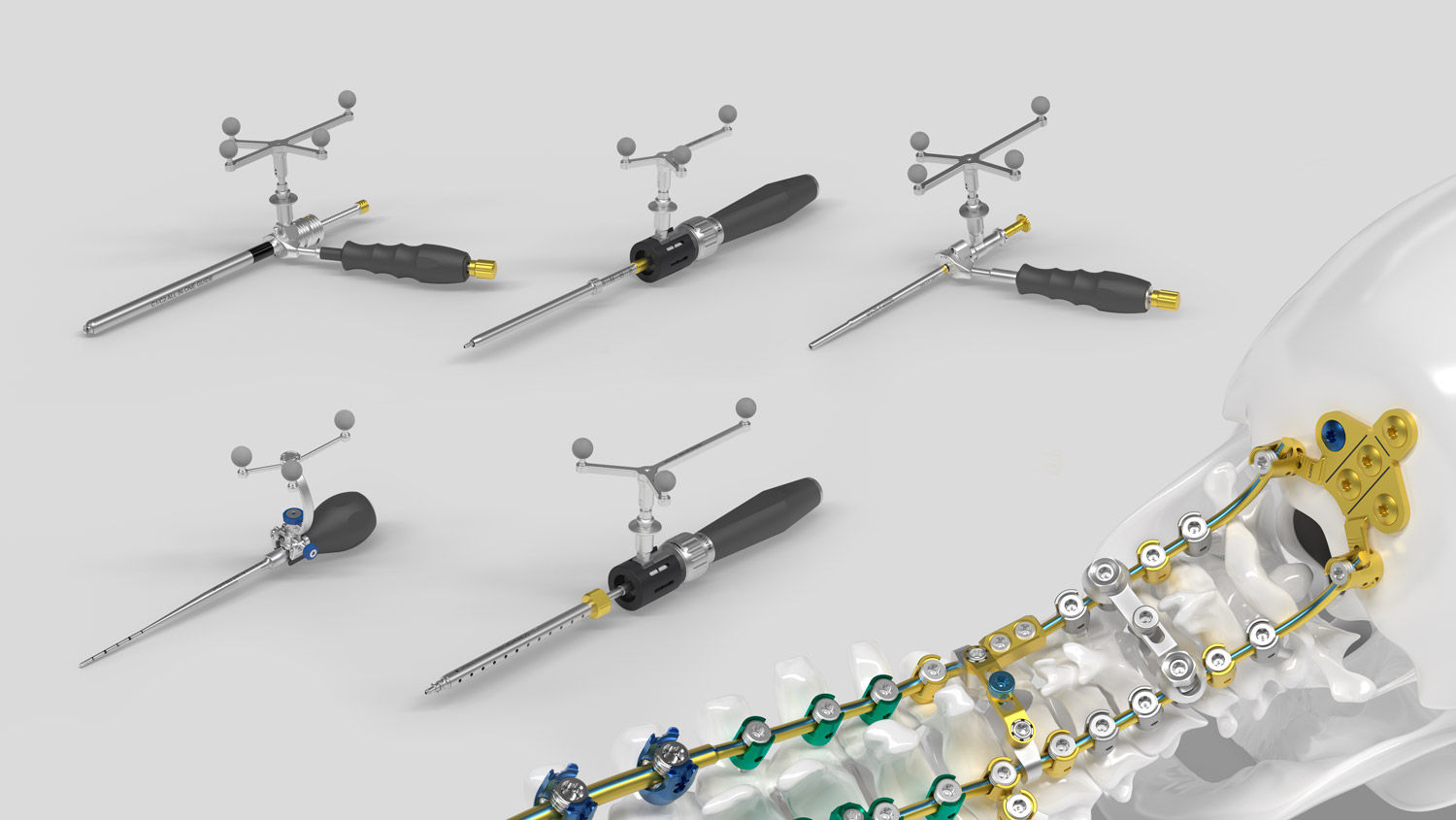
Ennovate® Cervical spinal navigation
The instrumentation is designed to allow for navigation without the need of an additional set of dedicated navigation instruments such as screwdriver or tap. The standard instrumentation may be navigated using the dedicated navigation handles and specifically designed interfaces on the instruments. Reducing the number instruments. Supporting your workflows.
Discover Ennovate®
[1] Kim D-Y, Lee S-H, Chung SK, Lee H-Y. Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation. Spine (Phila Pa 1976). 2005;30(1):123-9.
[2] Ringel F, Stoffel M, Stüer C, Meyer B. Minimally invasive transmuscular pedicle screw fixation of the thoracic and lumbar spine. Neurosurgery. 2006; 59(4 Suppl 2):ONS361-6; discussion ONS366-7.
[3] Lee S-H, Choi W-G, Lim S-R, Kang H-Y, Shin S-W. Minimally invasive anterior lumbar interbody fusion followed by percutaneous pedicle screw fixation for isthmic spondylolisthesis. Spine J. 2004;4(6):644-9.
[4] Sun X-Y, Zhang X-N, Hai Y. Percutaneous versus traditional and paraspinal posterior open approaches for treatment of thoracolumbar fractures without neurologic deficit: a meta-analysis. Eur Spine J 2017; 26(5):1418-31.
[5] Fong S, Duplessis S. Minimally invasive lateral mass plating in the treatment of posterior cervical trauma: surgical technique. J Spinal Disord Tech. 2005;18(3):224-8.
[6] Holly LT, Foley KT. Percutaneous placement of posterior cervical screws using three-dimensional fluoroscopy. Spine (Phila Pa 1976). 2006; 31(5):536-40; discussion 541.
[7] Scheufler K-M, Kirsch E. Percutaneous multilevel decompressive laminectomy, foraminotomy, and instrumented fusion for cervical spondylotic radiculopathy and myelopathy: assessment of feasibility and surgical technique. J Neurosurg Spine. 2007; 7(5):514-20.
[8] Thongtrangan I, Le H, Park J, Kim DH. Minimally invasive spinal surgery: a historical perspective. Neurosurg Focus. 2004;16(1):E13.
[9] Wang MY, Levi ADO. Minimally invasive lateral mass screw fixation in the cervical spine: initial clinical experience with longterm follow-up. Neurosurgery. 2006;58(5):907-12; discussion 907-12.


